Hey friends. Long overdue headache update comin' atcha! Head on over to my new Substack to read:
kathryndalton.substack.com/p/14-year-headache-update-neurostimulator
Hey friends. Long overdue headache update comin' atcha! Head on over to my new Substack to read:
kathryndalton.substack.com/p/14-year-headache-update-neurostimulator
Here I am, long overdue for an update yet again. So how are things going over here? Well, iIf my five year old daughter, Ryan, could sum it up for you, she’d likely throw her little fingers up into the most confident air quotes you’ve ever seen and say “Mommy’s head has felt soooo good these last seven months.” She’s still working through the nuances of sarcasm and irony but in this particular instance, well….she ain’t wrong.
The truth is, these last 6 months (9 months…12 months) have been filled with some of the worst pain days of the last 13 years. And given what the last decade + has been like, that’s a real gut punch just to type. For no identifiable reason, my headache has been so terrifyingly out of control. I can’t even think of another way to say it. It’s also been a very challenging few months working through one insurance denial after another, which I’ll get into.
In my last post last March, I recapped my trip to Park City to see Dr. Kutcher, the neurologist I’d been working with for the past 2.5 years. When I returned home to Arizona, I continued working remotely with his vestibular physical therapist, but the vestibular rehab was wrecking absolute havoc on my headache. That could be a positive indication that those systems are in play, but by the end of spring we had all decided it needed to take a backseat just so I could regain baseline function.
I’ve responded similarly to vestibular work in the past so it wasn’t entirely surprising, but incredibly frustrating nonetheless; to be working so hard just to gain an inch of traction and instead slipping, slipping, slipping further into pain that feels so inescapable.
Here are a few snapshots of pain flares in action. These skin changes on my neck are indicative of of the CRPS that gets triggered during some (but not all) of my worst increases in head pain. Cute, right?


By the end of March, I had completely stopped ketamine. We had a few new medications to try though - just anything to make even the smallest dent in my headache would be a win. Though I typically don’t have adverse reactions to most that I try, a few of these didn’t end well for me. First up was an anti-seizure drug called Lamictal, which is one of those meds you start at a low dose and gradually ramp up. That didn’t help and actually gave me hives (not the best, not the worst). Side note: If you're new here, I don't have (and never have had) seizures but these kind of anticonvulsants are often used to treat chronic pain because they help regulate abnormal electrical activity in the nervous system, which is also implicated in neuropathic pain, where damaged nerves send excessive pain signals to the brain.
There were two more antiepileptics. The first was Keppra, which provided nothing aside from a whole lot of fatigue and then, Oxcarbazepine. Oh, Oxcarbazepine. That one caused quite a bit of nausea and by the end of week one, I was headed straight from the parking lot of Ryan’s Sunday morning soccer practice to the emergency room. I’ve never thrown up more in my entire life. And that level of throwing up took my head to a level of pain where I was barely conscious. “Fun times” Ryan might tell you.
Mid-spring, I had gotten some Botox (just because it had been quite a few years and felt like it couldn’t hurt to try again) but after the second round a few months later, Dr. Kutcher suspected I could be experiencing a flare due to its wear off. I mean, that doesn’t feel fair.
Through the summer, I tried an abortive analgesic called Fioricet, in combination with Toradol. Many years ago, Dr. Dodick at Mayo would sometimes write me a prescription for Toradol (a non-steroidal anti-inflammatory) that Craig would inject. During super intense pain flares, the Toradol, albeit temporary, would sometimes help take the edge off. Unfortunately, not the case at all this time around.
Then there was Quilipta, an anti-CGRP migraine drug (also known as an CGRP inhibitor or CGRP antagonist). This class of migraine meds that are supposed to treat the pain by blocking the activity of a protein called calcitonin gene-related peptide (CGRP), which is thought to play a significant role in triggering migraine pain by causing inflammation in the membranes surrounding the brain. These medications bind to CGRP or its receptors to effectively prevent the activation of pain pathways. Some are abortive but most are preventative.
It’s sort of wild to reflect on the evolution of migraine medicine in the 13 years I’ve suffered. I remember sitting at Mayo with Dr. Dodick back in 2012 and hearing about these new medications that would be gaining FDA approval in the coming years. And If you’ve been following along for a while, you might recall that I’ve tried several CGRP antagonists before.
Over the past few years, I’ve been on Ajovy, Aimovig, Nurtec, Ubrelvy, and Zavzpret. Obviously none have helped me, but patients can respond very differently to each which is why you can’t write off the entire class of meds based on your experience with just one.
The fatigue I experienced from Quilipta was no joke, especially coupled with my sky high pain levels. I was struggling to make it to Ryan’s 7pm bedtime, crawling into bed myself as soon as she was asleep. It’s one thing to endure an unwanted side effect when a medication IS helping, but it’s really shitty to be experiencing those downsides when the medication isn’t even touching your pain. It feels like being kicked when you’re down and not even having the energy to get back up.
Most recently (just last week), II tried yet another CGRP drug called Vyepti. Vyepti is a once-every-3 months infusion, whereas the others have been either injectable or oral medications. I was able to have Vyepti administered by a nurse here at home, which was at least convenient. IV pole to my right and my Charlie girl curled up at my feet. So far, I haven’t felt any benefit but possibly still too soon to write it off.

The last medication worth mentioning is an Oxytocin nasal spray. There's some interesting research to support oxytocin as a modulator of pain perception and a natural pain reliever due to its analgesic properties and ability to reduce stress and anxiety associated with chronic pain. Oxytocin interacts with pain pathways in the brain, potentially by activating the endogenous opioid system, leading to pain reduction. And the most direct way to deliver oxytocin to the brain is intranasal spray. I've been using this prescription spray for a couple of weeks now. So far I can't say I've felt anything but the dosage is gradually titrated so we'll see if I notice anything. Can't hurt to try.
So now rewind for a minute back to April/May. Craig and I met remotely with a new doctor based in Dallas, Dr. Kenneth Reed of US Migraine (now Reed Migraine). Dr. Reed is the inventor of the “Reed Procedure” for migraine treatment. Simply put, the Reed Procedure involves implanting a small device under the skin near the occipital nerve, which delivers mild electrical pulses to disrupt pain signals and alleviate severe chronic migraines in patients who haven’t responded to other treatments (hi, it’s me!). It works by targeting the nerves in the supraorbital and occipital regions of the head (hi, it’s my headache!)
It wasn’t that this procedure has never been on our radar. We actually spoke to Dr. Dodick at about it a decade ago but at that time, implanted neurostimulators for chronic headache involved wire leads running under the skin up along the spine and I was told that it would likely have an effect on my ability to be active.
Craig and I had a really thorough and thoughtful conversation with Dr. Reed. He explained that patients first undergo a temporary TRIAL stimulator first to ensure that the procedure works for them before fully committing to the permanent implant. During the trial, they implant a temporary unit underneath the skin (similar to an IV tube) which stays in for just 3-7 days. I’d stay in Dallas during that time and have it removed before flying back to Arizona. For patients who experience relief with the trial, the effects are typically dramatic, which allows them to make a decision of whether or not to proceed with the permanent stimulator with a good deal of confidence.
For the permanent stimulator procedure (which would be on a separate trip), two leads are superficially implanted right underneath the skin along the supraorbital nerves above each eyebrow.

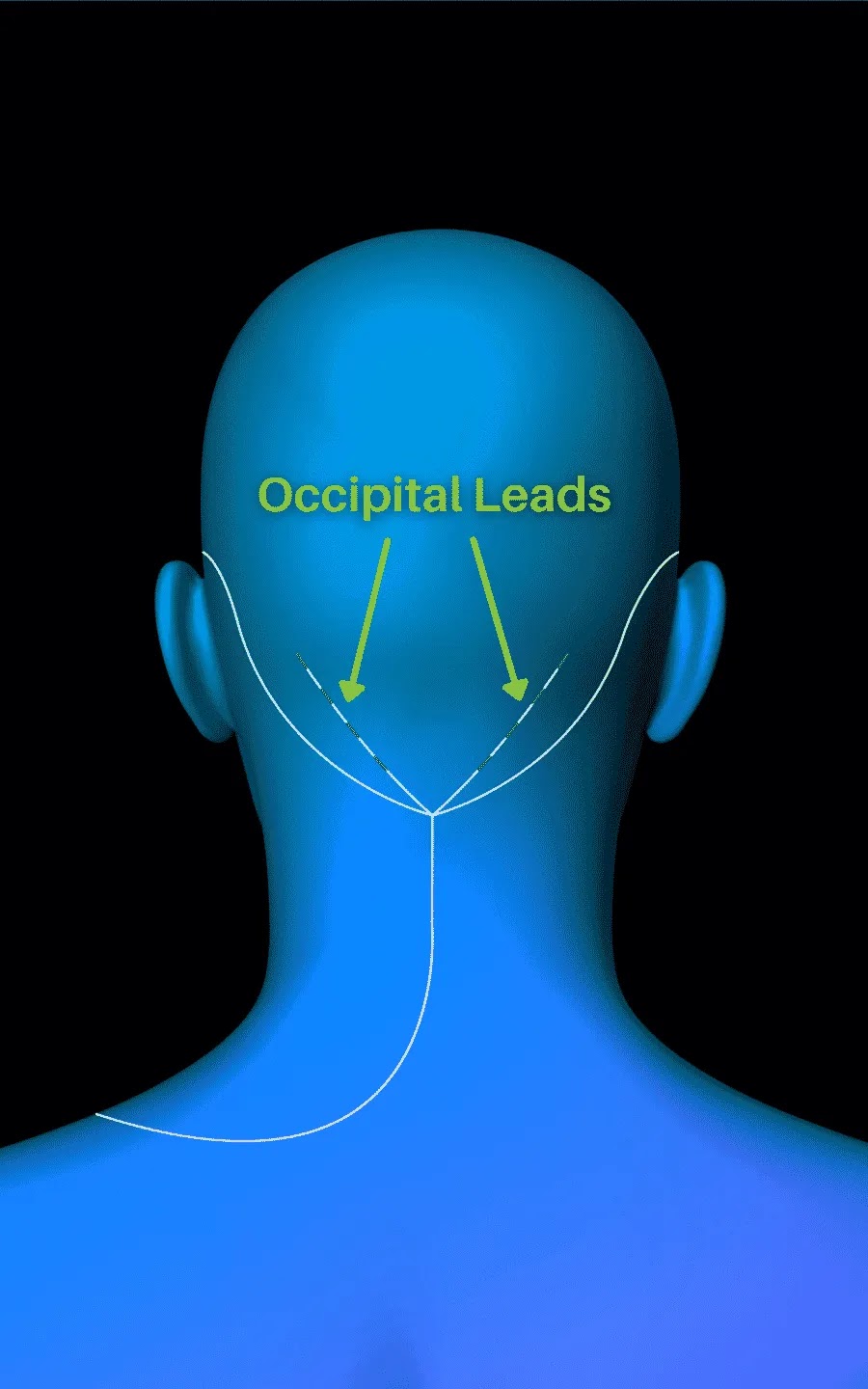
Two leads are superficially implanted right underneath the skin along the occipital nerves in the back of the head.
And a battery/pulse generator device is superficially implanted right underneath the skin on the left side of the chest.

Even though the leads, battery, and connecting wires are right under the skin, they’re not at all externally visible so you would never know by looking at someone that all this magic is happening just beneath the surface. Honestly though, if it took my pain away, I’d proudly rock that look all day every day.
There was no doubt from Dr. Reed that I’m a prime candidate for the surgery. And from my perspective, it also feels like there’s not a whole lot to lose moving forward with the trial. If it works, life changing. If it doesn’t, I’m not worse off than I am now. Reed Migraine states that the stimulator does work for over 80% of their patients, which is very encouraging. But I’ve also learned not to get too attached to stats and success rates and just take it one step at a time.
Here’s where things got a little bumpy for us. As soon as we had that phone call with Dr. Reed and had all my records sent over, we began the pre-authorization process. Over the course of thirteen years, Craig and I have been through the ringer with insurance. And as you might guess given every treatment/therapy that I’ve pursued, there has been quite a lot that we’ve come out of pocket for. But even the majority of medications and procedures that have been covered have only been approved after initial denials, appeals, more denials, peer-to-peer reviews, etc. And hey, I get that those systems are in place for a reason and I don’t think I’m an exception to the rule. But the shit we’ve been through trying to get treatments approved is absurd. For example, several years ago I was having a nerve block done under CT guidance. The procedure was denied, appealed, and ultimately approved. My pain management doctor opted to perform each side on different days for both safety reasons and to better identify a pain source (so technically they were treated as separate procedures). After the whole rigmarole of getting the first one approved and performed, the second side was denied and we had to restart the whole appeal process. That just paints you a little picture of what we're working with here.
Or take the Yvepti infusion I had just last week. It was submitted to insurance along with 65 pages of my headache treatment history from my neurologist. I received a denial letter saying:

I haven’t had more than 4 migraines per month? How about every day of every month for approximately 160 months and detailed medical records documenting 13 years of treatment? What the actual fuck.
The letter goes on to explain that Yvepti is only considered medically necessary if I’ve tried (without success) the other anti-CGRP drugs and then goes on to list Ajovy, Aimovig, Nurtec, and Ubrelvy. Do you remember a few paragraphs ago when I listed those CGRP medications as ones I've tried in the last 2 years? If so, congratulations - you've already read more than the person whose literal job it is to review my required medical history and determine the fate of my treatment. Back through the appeal process we went and fortunately, Yvepti was ultimately approved.
My intention in rehashing this isn’t to dwell on bullshit I obviously have no control over. I like to think that it’s not in my nature (or Craig’s) to assume the worst of others’ intentions, but it is just mind numbingly insane to me that it is someone’s job to review my records and make a decision on very objective criteria and they can just fail at it so hard. And all at the expense of my pain. I would love nothing more than to stand face to face with an individual who is making these determinations and ask them to consider the human being on the receiving end; to ask them to imagine if that person suffering was their wife, husband, child, or parent.
Anyway, sometimes the appeal process IS fairly straightforward, but in the case of this Reed Procedure, it’s taken approximately 7 frustrating months. Fortunately, Craig is (and always has been) my biggest advocate and he takes this all head on. If you only knew the hours he’s spent on the phone with the insurance company, the case managers, the benefits team, the doctors offices, the attorney, trying to sort it all out. It makes me feel so grateful for him but also infuriated that this is the system people in my position have to fight against. Chronic pain warriors, many of who struggle just to get through the day, have to battle the very insurance companies we are PAYING customers of, just to get the care we need. And sometimes even then, it’s still not enough.
Obviously our goal was to not be paying cash for this surgery. We fought through appeals, the clinic resubmitted under several codes since I technically have more than one diagnosis (including complex regional pain syndrome), and through each step of the process, the insurance company maxed or exceeded their “response window” before sending the rejection. The last step was an external review, which was ultimately denied just a few weeks ago. So that really blows.
The positive is, we are moving forward with the Reed Procedure regardless. And another positive is that we pay up front for both the trial and the permanent implant but if the trial doesn’t work for me, we get a complete refund. That is not even close to common practice, and is one more reason we feel so confident in giving this thing a shot. If it doesn't work, I'll know I've given it a fair shot and if it does work, it'll be the best money we've ever spent and maybe will ever spend in our lives. Cautiously optimistic as ever.
My trial is scheduled for early January. So Craig, Ryan, and I will head to Dallas for about 5 days. I'll get all wired up on a Tuesday morning and sort of go about the next few days as normal. For patients that have identifiable triggers, they're advised to lean in to all the things that spike their pain with the temporary stimulator. For me, that shouldn't be an issue. Then it'll be removed on Friday and FINGERS CROSSED, I'll be elated with the outcome and the surgery can be scheduled not long after.
I'll update more from Dallas!
A long overdue headache post comin' atcha.

When I last updated in June, I talked about microdosing with psilocybin (i.e. mushrooms). I called it quits on that after a month or so. It wasn't making a dent in my pain levels at all and oddly enough, seemed to actually be making me feel worse. How?? Considering the proposed mechanism of psychedelics on the body's serotonin receptors, it makes very little sense that they could make my headache worse. But then again, medical mystery is kind of on brand for me.
In June, I was also getting ready to head back to Denver for another procedure. As you might remember, I had been seeing Dr. Callen who heads the CSF Leak program at UC Health University of Colorado Hospital. Though no imaging to date had pointed to me having a dural tear that could be causing a leak of my cerebral spinal fluid, there was a chance that an MRI myelogram could tell a differently story.
An MRI mylogram is where they insert a needle into the spinal canal and inject a contrast material into the subarachnoid space using fluoroscopy (a real-time form of x-ray) to get a more detailed picture of the spinal cord, nerve roots, subarachnoid space, and spinal column. The plan, after that, was for me to have a blood patch performed. You can refer back to my previous post if you want to learn more about what that consists of.
In early summer, sometime between my last trip to Colorado and my scheduled return trip, I had begun working remotely with a new neurologist, Dr. Kutcher, with the Kutcher Clinic for Sports Neurology. This is a doctor we were connected with through Craig's work - he works with many elite athletes and as an advisor to the NFL Players' Association. In my initial appointments with him, it was clear that Dr. Kutcher wasn't super keen to the idea of a blood patch, concerned (understandably so) there was a chance it could make my symptoms worse. With such a seemingly low probability of a leak, I was leaning towards putting that plan on pause, at least until I had tried a few things with Dr. Kutcher.
But then one early morning in late July (Craig's 50th birthday to be exact!) I had a total random fall hopping off a bench while working out in our garage and broke my foot. I basically just landed on the side of my foot, then fell into (and crushed) a metal box fan. Silly me! Just trying to keep things interesting. I would need surgery the following week - a screw inserted to fixate a fractured fifth metatarsal. At that point, the Denver trip was delayed whether I wanted it to be or not. The whole foot ordeal ended up being quite a speed bump - or series of speedbumps - over the next few months, but I'll get back to that.
I will say, though, spending just a few short months with an injury so visible to the outside world was such a harsh reminder for me of just how invisible my headache really is - the pain that is so, so, SO much worse than any broken bone could ever be. Just the idea that needing to wear a boot on my foot or get around on crutches would be disruptive to my life feels laughable when I consider how my head pain affects how I move through the world. Ooof.
So anyway, I spent June doing a bit of a treatment reset with Dr. Kutcher. After taking an extensive case history (no small feat), his simplified perspective was that my head pain is not caused by one single driver right now. Yes, there is surely central sensitization at play - a pain loop that's proven incredibly difficult to "turn off." Yes, the topical skin changes (new pics below) appear to be evidence of complex regional pain syndrome (CRPS). Yes, the nerves in my neck are contributing. The pain is central, the pain is peripheral - it isn't a case of either/or. Not really new information, but validation nonetheless.



Dr. Kutcher pointed out that although I've been on a lot of meds over the years (both traditional migraine medications along with others that target the central sensitization/neuropathic pain), there were some missing from the list. First though, he wanted me to do a GeneSight Psychotropic test, which is a blood test that analyzes how your specific genes may affect the outcomes of different medications - a simple test that allows for a much more targeted approach to medications, compared to the conventional trial-and-error process. It's especially impactful when you consider how expensive and time-consuming trying different drugs can be. It can often takes weeks or even months to work up to the right dose, give your body a chance to respond, and even taper off if deemed ineffective.
So anyway, I did that test and we started working through some different medications. There was Nurtec, then Ubrelvy, then Zavzpret, which are all calcitonon gene-related peptide (CGRP) receptor blockers aimed at treating migraines. But no dice. And these wasn't my first go CGRP inhibitors. Having already eliminated Aimovig and Ajovy injections, we agreed I'd officially exhausted this class of medications. Then there was Nortryptaline, a tricyclic antidepressant used off label to treat chronic pain. That one came with some ick side effects for me, mostly nausea (but more importantly, no pain reduction).
Right around this time (early August) I was experiencing massive (f-ing MASSIVE) pain spikes due in large part to my foot surgery. One thing I've learned over the years is just how poorly my head responds to extra inflammation/trauma in my body, from the most simple things like colds/flus/vaccines to more severe like surgeries, childbirth, mastitis, etc. So between breaking the bone, the surgery, and a horrible reaction to the Oxycodone I was given, my head was just absolutely out of control. Unfortunately, that trend continued through the fall.
I was trying any little thing I could to bring my body into balance - continuing my workouts, daily cold plunging, and a biofeedback technique called HeartMath. Based on the notion that heart rate patterns can affect your mental state just as much as your mental state can affect your physicality. HeartMath uses coherence technology. It's pretty simple - you attach this little device to your body that measures your heart rate variability (HRV), which is a measure of the time variation between heartbeats. HRV is regulated by the autonomic nervous system (ANS). The ANS has an important role in the body's physical response to stress. Specifically, the sympathetic nervous system (SNS), is responsible for the "fight or flight" response. When you live in chronic and persistent pain, your body's "fight or flight" mode never gets turned off. The goal of Heartmath Biofeedback is to learn to change your heart rhythm to create physiological coherence, to help you feel less alarm and more calm.
Then in November, I began a course of at-home ketamine treatments. Not my first special K rodeo, but it had been almost a decade since my infusions. For those unfamiliar with it, Ketamine is a dissociative anesthetic. At sub-anesthetic doses, it can be used to help treatment-resistant depression along with acute and severe pain. But it also shows promise in treating chronic pain, particularly neuropathic pain, which is just is a whole other beast. It's been shown to benefit patients suffering from central sensitization and complex regional pain syndrome (CRSP), which we know are at least partial contributors to my chronic head pain. Though the infusions back in 2014 didn't do much to help me, it felt like perhaps it was worth revisiting.
This time, though, I started with oral ketamine. I opted for sublingual tablets versus jumping straight back into intravenous for a few reasons: I didn't tolerate the IV super well, whereas this is a lower dose. That also makes it more cost effective and a lot more convenient. In November, I began with two sessions per week and was able to schedule them on days where Craig was able to pick Ryan up from school, as it wouldn't be safe for me to drive for the rest of the day.
My at-home sessions looked like this: Thirty minutes after taking an anti-nausea med, I would get into bed (bedroom blacked out) and place the tablet or troche under my tongue. (I worked up to my prescribed dose over the first few sessions.) I would let the tablet dissolve in my mouth and then keep my mouth closed for about 15 minutes without swallowing. Then I'd spit it all out into a cup. Seems like an odd way to take medicine but the reasoning here is that when you swallow ketamine, it undergoes first-pass metabolism in the stomach and liver, where it's converted to something called norketamine. Norketamine, though still psychoactive, isn't as potent as ketamine. If you do swallow it, you'd likely need a higher dose to achieve the same the same therapeutic effect.
So anyway, around the time that I'm spitting it out is when I'm starting to feel...mmm, on drugs? I quickly get my earbuds in and click "play" on the recommended Spotify playlist, close my eyes, and relax my head onto a cold icepack atop my pillow (the ice is my personal touch - I never lay in bed without it). What happens from there is hard to describe and it does change a bit from one session to the next. The first day I really hated it. I've never enjoyed feeling like my mind is entering an altered state and there's nothing I can do to stop it. But it's gotten much easier with subsequent treatments, now that I have some general expectations. It feels a little like dreaming without being asleep. A trance-like state, I guess. The "high" lasts only about an hour for me, though I usually turn off the music and try to sleep or at least rest in bed for an additional 45-60 minutes. I feel pretty gross for the next few hours, though. Wiped out and a little hungover feeling. But that seems to subside by the next morning.
I finished up my course of Ketamine treatment by early December but was unsure of whether to continue. I was sort of having a more normal (ie baseline pain) few weeks, but there seemed to have been so many other variables affecting my pain leading up to that too, so it was hard to know. And there was about to be another hiccup.
After several months of physical therapy, my foot wasn't healing super well and it was clear that the screw needed to come out. Again, totally straightforward surgery but it took another huge toll on my head. This time, I wasn't touching a pain killer but that didn't seem to matter. And then the week after, I came down with an upper respiratory infection that progressed to pneumonia. All things that are a nuisance but it was like my headache was just taking one hit after another. And once my pain had reached this peak, it was just unrelenting. January was one of the hardest headache months I've had in the last 13 years. I was waking up in the morning and falling asleep at night at a level of pain that has been reserved for the worst moments of my worst days. Completely unsustainable but also....what was option B? We had some really stormy weeks here too, and as much as I crave a cloudy day in the desert, the shifting barometric pressure was adding fuel to the fire.
Towards the end of January, Craig had something called the Ammortal Chamber come to his work that I tried out for a few sessions, hoping it might help break this cycle I was stuck in. It uses a combination of pulsed electric field (PEF)/pulsed electromagnetic field (PEMF), red light photobiomodulation, molecular hydrogen, and vibroacoustic therapy. Super relaxing. And defying all odds, my headache spiked even more. (Actually not my first time I've had a negative response to red light therapy, which baffles any practitioner I talk to due to the ability of red light to increase blood flow and reduce inflammation.) Again, it makes very little sense how that could worsen my headache.
In mid February, I decided to start a second round of weekly ketamine. Though some people do have profound and fairly immediate relief from Ketamine therapy, it also isn't uncommon for it to take more time. And now that I had some distance from my surgeries, I wanted to give it one more shot.
Then that brings me to early March, when I traveled to Park City to meet with Dr. Kutcher in person. Telemedicine is so wonderful, but there are some things that just can't be accomplished with a screen between you.
One of the reasons Dr. Kutcher wanted to see me in person was for some cognitive testing. My palms get sweaty just writing those words, so you can imagine how imagine how I feel going into it, hah! All kidding aside, the testing we did was quick and painless (nowhere near as draining as all of the brain mapping I had done a while back at the Brain Resource Center in NYC.) He uses an assessment tool called NeuroCatch, which evaluates brain activity using event-related potentials (ERPs).
"ERPs are long-standing extensively studied brain activity responses linked to cognitive function. These vital responses allow for objective evaluation of Auditory sensory, Basic attention, and Cognitive processing, which can be used to optimize individual brain health and guide brain care in conditions like brain injury, mental health disorders, and neurological diseases.
ERPs are a “brain fingerprint” of cognition. They have been rigorously studied and validated in over 150,000 medical publications. They increase the accuracy of existing subjective cognitive evaluations. They are sensitive to external factors such as sleep, stress, and fatigue/inattention[1]; yet they are impervious to user bias that attempts to hide the effects of a head injury, for instance."

So how did I do?
Much to my surprise, pretty good. From an auditory and cognitive processing standpoint, my amplitude was fine and my latency was quick. He was actually a little taken aback by how quick and explained that the brain responding "too quickly" could potentially indicate that the wrong areas are firing.
Next, I headed into the gym for what was arguably the least pleasant part of my visit. The goal here was to taken me through a series of exercises that would purposely flare my symptoms by overstimulating my brain. Here was the recipe for that fun experiment:
1. Music turned on
2. Me, standing in in a 4-square layout on the gym floor, following instructions to jump forward, back, jump 180 degrees, jump 360 degrees
2. While following jumping instructions, counting backwards from 100 to zero by multiples of 7
3. While following jumping instructions, catching a multi-colored object with whichever hand was called out by whichever colored portion of the object that was called out
Let me just pause here and remind you that when my pain levels are spiked, my brain feels like it will explode if two people start talking to me at one time. So it goes without saying that this part of the afternoon really...fucked me up.
Which was the goal! Because next my eye movements were assessed again to measure any chances with an increase in pain and general feelings of dizziness. And they weren't majorly affected. This indicated that visual input doesn't seem to be a major driver and the inefficiency of my vestibular system is a more likely culprit.
He also had me take 2 Nurtec that evening (one of the CGRP migraine abortives I had tried months ago) just to see if made any sort of dent (which it did not).
So overall, what information did all of this testing provide? According to Dr. Kutcher, there are two primary "flavors" of central pain: hypersensitivity (meaning the part of your brain that processes pain is super efficient at doing so) and structural changes. He thinks that for me, hypersensitivity is a bigger issue than structural changes. So where medications like serotonin uptake inhibitors and even drugs like Ketamine are still worth pursuing in an effort to make structural brain changes, retraining of the brain through vestibular therapy will be most important for me.
On my second day at the Kutcher Clinic, I met with the vestibular physical therapist. His assessments made it pretty darn clear how off my vestibular system is. As an example, he'd have me do things like stand and look at the wall in front of me, close my eyes, then have me turn around and stop/open my eyes when I thought I had returned to my starting position. I didn't excel here, to put things lightly. You would have thought I was failing a roadside sobriety test.
So the plan right now is to focus on some proprioceptive work in an effort to recalibrate my vestibular system. I have a program to do from home that consists of basic eyes-closed movements and sensory motor control exercises, like using a laser attached to my forehead to trace my eye movements through this maze while balancing on one foot, moving forward/backward, side to side, etc.

I've seen vestibular specialists at Mayo before, but that was well over a decade ago and at that time, it was more to rule certain things out. This will be my first time really focused on a vestibular rehab program.
Dr. Kutcher agreed I should finish out this current Ketamine protocol (yesterday was my last day on it) and if there's been no improvement (which there's not seeming to be), he'd like me to try a medication called Lamictil (an anti-seizure med but another that's used off label for neuropathic pain). He also did a series of anti-inflammatory trigger point injections just to see if those would do anything. I've obviously had injections like these many times before so we weren't super optimistic. And they didn't do anything.
I think that about sums it up for now. I'm hopeful that this vestibular rehab will be a step in the right direction at the very least. Just one step is all I need right now.
And since I always like to leave it on a happy note, signing off with this one. She might be part of the reason I'm exhausted by 7pm but she's definitely the one who gives me energy to get through my hardest days. The brightest light for me (and anyone who meets her).

Earlier this week, I returned from Denver. I was there for a consultation with Dr. Andrew Callen, neuroradiologist and director of the CSF Leak Program at UCHealth University of Colorado Hospital. I realized on the trip that I was long overdue for a blog post. It's been 9 whole months since the last update, and I guess I've been putting it off waiting for some incredible breakthrough to report. Have I learned nothing?
When I started writing this blog in 2013, it was intended as a way of updating friends and family about the treatments I was pursuing for the post-traumatic headache I had sustained a year and a half prior. The headache I was taking a "temporary" leave of absence from my job to tackle head on (pun intended).
Next week marks 12 years. My headache is a fucking preteen. I can hardly stop long enough to let that sink in. Mostly because I can't afford to let it bring me down. My physical pain has got that one covered.
The last six months have been hard. Really, really hard. Pain levels spike but don't come down. Baseline "norms'' are recalibrated and the cycle continues. There have been many nights this year where I've laid in bed, numb with ice packs from the base of my skull to my eye sockets, contemplating a trip to the ER before inevitably deciding I can't possibly sit in a waiting room for who knows how many hours only to be given an infusion that does. not. help. I'm honestly not sure which is worse: falling asleep to the feeling of a drill going through my temples or waking up the next morning enveloped in the same agony. Agony that is entirely consuming of my life yet equally invisible to the world around me.
A few months back, I was listening to this podcast discussion about the topic of "loving your body." The hosts were discussing the topic within the context of body image, but it struck a real cord with me nonetheless. Made me think about my (complex) relationship with my own body. There's this quote from Glennon Doyle. She says, "Your body is not your masterpiece - your life is…
...It is suggested to us a million times a day that our BODIES are PROJECTS. They aren’t. Our lives are. Our spirituality is. Our relationships are. Our work is. Stop spending all day obsessing, cursing, perfecting your body like it’s all you’ve got to offer the world. Your body is not your art, it’s your paintbrush. Whether your paintbrush is a tall paintbrush or a thin paintbrush or a stocky paintbrush or a scratched up paintbrush is completely irrelevant. What is relevant is that YOU HAVE A PAINTBRUSH which can be used to transfer your insides onto the canvas of your life — where others can see it and be inspired and comforted by it. Your body is not your offering. It’s just a really amazing instrument which you can use to create your offering each day. Don’t curse your paintbrush. Don’t sit in a corner wishing you had a different paintbrush. You’re wasting time. You’ve got the one you got. Be grateful, because without it you’d have nothing with which to paint your life’s work. Your life’s work is the love you give and receive — and your body is the instrument you use to accept and offer love on your soul’s behalf. It’s a system."
What a poignant perspective, right? I can almost feel myself nodding along just reading that. Except that... when you live in pain...when pain infiltrates every waking (and sleeping) moment of your existence, where does your body end and your life begin? Where does your pain end and your body begin?
It is fucking messy. And it's something that I struggle with every day. I can repeat positive mantras like "I am not my pain" all day long, but my head pain physically exists inside my skull. How do I reconcile that my own body is both the hero and the villain of the same story? That it's both capable of and responsible for defeating this thing that in so many ways, steers the ship. How do I muster the emotional, mental, and physical strength to fight something while simultaneously making peace with my own reality? I don't have the answers. But I suppose it's why I keep trying to prove to myself that this physical body I am moving through the world in is good, is able, is strong, even when (especially when) my pain is screaming otherwise. The fake-it-til-you-make-it brand of resilience, I guess.
To be totally honest, every treatment/therapy/medication that I burn through really takes a toll. An emotional rollercoaster of hope and defeat, hope and defeat. Even still, the landscape of headache medicine (especially given the 12 years I've suffered) is ever evolving, and it keeps me optimistic to learn about new developments in the treatment of this debilitating disease.
One of those treatments is psychedelics. As you may well be aware, there's been an absolute explosion of new research into a wide range of therapeutic uses for psychedelics. And chronic pain and migraine/cluster headaches have been one really interesting area of focus. You may remember reading about my ketamine infusion back in 2014 (fucking wild, by the way). But until recently, I had zero experience with microdosing.
Microdosing, by definition, is the practice of consuming very low, sub-hallucinogenic doses of a psychedelic substance. In the case of psilocybin mushrooms, that's 0.1-0.4 g. The tough thing (aside from the obvious challenge of accessibility due to the fact that they're not yet legal), is there's just a lot of trial and error involved. Strain, dosage, frequency, time of day - you know, all of the known variables we take for granted with prescription medications. So I haven't thrown in the towel yet, but I certainly haven't felt any benefit either.
If you're interested in learning more about psychedelics and chronic pain, here are a few articles to start:
Repeat Dosing of Psilocybin in Migraine Headache
Yale Research on Psychedelics Gives Hope to Headache Disorder Community
Are psychedelics the answer to chronic pain: A review of current literature
So Dr. Callen leads a collaborative team of radiologists, neurologists, and neurosurgeons to provide cutting-edge testing and treatment for those suffering from the condition. Like I mentioned, long held belief in neurology has been that a CSF leak is ruled out by a normal brain MRI. (It's the reason that it was crossed off the list for me at Mayo over a decade ago.) Only since 2014 has a type of called a CSF-venous fistula (CVF) been discovered.
To clarify, spinal CSF leaks originate from dural weakness (dura is the outermost layer of connective tissue that surrounds the brain and spinal cord) and meningeal diverticula at the surrounding nerve root sleves (which are called cerebrospinal fluid-venous fistulas, or CVFs). Located mainly located in the thoracic region, CVFs are defined as "abnormal connections between the spinal subarachnoid space and adjacent paraspinal veins that allow unregulated egress of CSF into the venous system." Cerebrospinal fluid (CSF) venous fistulas are a recently discovered and underdiagnosed cause of spontaneous spinal CSF leak, which may lead to spontaneous intracranial hypotension.
Over the last year, I've continued to show signs of complex regional pain syndrome (CRPS), which manifests through these topical skin changes. Here - I'll throw a collage in just for fun. CRPS indicates a malfunction of the central and peripheral nervous systems and in my case, we think has developed as a result of my head pain persisting for so long. How messed up is that? The more chronic a pain condition becomes, the more sensitivity becomes central. It's a cycle proven incredibly difficult to break.
.jpg)
I don't experience these skin changes every time I'm in an incredibly severe head pain flare...but every time I experience skin changes I am in an incredibly severe head pain flare. It typically gets very blotchy and sometimes streaky - often concentrated at least to some extent in that spot on the left side. The skin sometimes peels and sometimes opens and just sort of feels like it's burned. So weird.
Now on to some treatment updates:
Last fall, I began seeing Dr. Rau. As member of the Spinal CSF Leak Foundation's advisory board, she's one of the few neurologists in the country really dialed in to the latest research and treatment of CSF (cerebral spinal fluid) leaks. She also just happens to be local, which has been great. While we were navigating the leak stuff, I began some other treatments with her.
After six years of fertility treatments, pregnancy, and breastfeeding, I've finally been able to try two different calcitonin gene-related peptide (CGRP) monoclonal antibodies, or CGRP inhibitors. CGRP inhibitors are drugs that block CGRP from binding to CGRP receptors, a key contributor to nerve pain and inflammation of migraine. Ajovy was the first one I tried. Here's an enthralling capture of my first at-home injection. I continued these for 3 months (no improvement) before Dr. Rau prescribed me another CGRP inhibitor called Aimovig. I'm due this week for my second round of Aimovig but so far....well, you can probably guess.
If you remember from my last post, I had consulted last year with Dr. Schievink, director of the CSF Leak program at Cedars-Sinai. After a review of my imaging, Dr. Schievink didn't see evidence of a dural tear. But Dr. Rau wasn't convinced it was worth writing off the possibility completely. Apparently, 20% of leaks show normal brain imagining, which is kind of shocking. That's why put me in touch with Dr. Callen and the CSF Leak program at UC Health University of Colorado Hospital.
Real quick, if you're wondering how exactly a dural tear and subsequent leak of CSF causes a headache, here's a good explanation from Johns Hopkins:
"The brain normally sits inside a bag filled with spinal fluid that extends down from the skull into the spine. The bag consists of membranes called the meninges (as in meningitis). The fluid helps to circulate waste products out of the brain and provides cushioning and support. When the pressure of this fluid is too low typically when there is a small leak somewhere in the meninges — the brain may sag downward when the patient is upright, stretching the meninges and nerves lining the brain and causing pain."
CVFs require a special type of testing called dynamic myelography to diagnose.
Despite not yet having a full workup, Dr. Callen has been honest with me. He's doubtful (but not certain) I have a leak. This shouldn't really surprise me, especially since there's never been orthostatic component to my pain (head pain worsening upon standing, improving with lying down). With that said, it seems like he knows enough to know there are few absolutes. He even said during our visit "This disease has humbled me." Though the probability is low, there is still a chance I am leaking. And when you've suffered this badly for as long as I have, you cling to single digit probabilities because sometimes that's all you have to cling to.
The plan right now is for me to travel back to Denver in late summer for an MRI myelogram. I've actually never had this specific type of imaging done before. Here's what will happen: they'll insert a spinal needle into my spinal canal and inject contrast material in the subarachnoid space using fluoroscopy (a real-time form of x-ray) to get a more detailed picture of the spinal cord, nerve roots, subarachnoid space, and spinal column. After that, I'll have a blood patch performed.
For the blood patch, I'll first get an IV inserted. Once in the procedure room, I'll have a CT-guided lumbar performed at a specific site. The blood they obtain from my IV will then be injected into the spinal needle in an attempt to "patch" a leak (if there is one). The tricky part will be the blood patch recovery. I'll need to lay as close to absolutely flat as possible for 72 hours (I can get up briefly to go to the bathroom and sit up to eat). If I don't feel an improvement in the weeks/first few months after my blood patch, we feel confident we can eliminate a leak once and for all and figure out what the next step is from there. As always, one day at a time.
Hi friends. It's been half a year since my last post. Six whole months since my stem cell procedure in Grand Cayman. So... did the long awaited intervention help? I'm devastated to say that as of now, no. Not even a little bit.
I hate more than anything to start this off on such a low note, but the last few months have been some of the most challenging of the last decade for me. The only way I can describe my head pain has been just out of control. But I'll get to that.
I'm thinking back to spring and it's sort of a blur. I worked through the recovery protocol from my March procedure. In my last post, I outlined the phases of tissue healing. Here now in month six, I'm closing in on the end of remodeling, when the tissue should be constantly improving to become stronger, functional, and closer to normal. Technically, full healing can take up to a year with peak functionality at 1-2 years, but full transparency: it's hard to feel optimistic at this point.
I returned to some physical therapy in those following months too to help return some necessary foundational strength and function to my cervical spine.
In April, I explored some form of structural integration therapy that didn't go well. It's not worth getting into the details, but suffice to say it was just another exhausting example of a practitioner trying to fit a complex problem into their sellable solution.
Not long after, I had a few appointments with a new physical therapist with a cranial sacral focus. She uses different manual techniques to access connective, visceral, neural, muscular, and fluid tissue. It's almost hard to believe my body could respond this way because the therapy is so incredibly gentle, but sure enough, it flared me right up. Horrible-electric-mixer-in-brain feeling. It's hard to even describe because it's so much more than pain. If you've been around since the beginning, you know that's exactly how I responded to cranial sacral back in 2013 - it's what led us to suspect a dural tear (the dura is the connective tissue that covers the brain and spinal cord) and check for a resulting cerebral spinal fluid (CSF) leak. That was ultimately ruled out with MRI.
I also consulted with Dr. Peled (my occipital nerve surgeon) about the possibility of trying another round of blocks to explore whether a frontal surgery was warranted. The pain in my supraorbital region (above my eyes) and temples has just been so, so intense. The problem is that the same level of pain is also widespread. Over the top of my head and down into suboccipitals. I just don't have a great degree of confidence right now that cutting those nerves in front would make a significant impact. And the reality is that even when we've identified damaged nerves, tissues, joints, I have had a favorable response to exactly ZERO procedures I've undergone over the course of 11 years. How is that even possible? So while I'll never be afraid to undergo another surgery, I can't say I'm overly hopeful either.
In July, Craig and I finally made it to the Brain Resource Center in NYC. (Our failed attempt last summer got us as far as the tarmac in Boston.) The BRC is a brain wellness and optimization treatment center. It's run by Dr. Fallahpour, a clinical psychologist and neuroscientist, who uses brain-computer interface technology and neuroscience research to treat a variety of psychological and neuropsychological disorders, including anxiety, depression, ADHD, chronic pain, and brain injuries.
We're working off the assumption that central sensitization is, at the very least, contributing in some way to my intractable chronic head pain. What that means, in a nutshell, is that when you're in chronic pain, the parts of your brain that experience that pain undergo physical changes. As more and more neurons are recruited, those pain processing regions become hypersensitized (essentially "better" at feeling pain). I guess you could think of this as the really shitty part of neuroplasticity, or the brain's ability to change and adapt as a result of an experience. Keep in mind, this isn't referring to the "mind" changing in some conscious way, rather, literal structural changes occurring in the brain. On the flip side, if the brain's structure can be changed through some sort of therapeutic intervention, central pain can be disrupted. That's really the idea behind this sort of treatment.
We spent a few days at the Brain Resource Center. The first day was the most "demanding" on this old noggin of mine. She certainly doesn't work like she used to, I'll tell you that much. I underwent a comprehensive brain map assessment (quantitative electroencephalography) to measure the electrical activity of my brain while engaged in a series of cognitive tasks. That gave them a visual representation of the parts of my brain that were over or underactive. And then based on those patterns, they designed a neurofeedback program that was intended to help me learn to rebalance my brain activity and ultimately/hopefully decrease my pain.
My brain map results showed two primary areas that are underactive. The first is my anterior cingulate cortex, likely due to pain and persistent attention to pain. This part of your brain is what directs and manages attention. So the more "tuned in" I am to my pain, the more that area physically grows. I work so hard (so f-ing hard) to stimulate my body and mind in ways that detract as much as humanly possible from my headache (example: the importance of my workouts) but emergency room level pain is just straight up impossible to "ignore." The second part was my sensorimotor cortex, which is involves in pain perception.
Sooo... yes, brain map checks out.
In terms of my cognitive performance tests, I scored in the normal range but my visual memory was lower. That's to be expected given how chronic pain affects memory. It also explains why my not-even-3-year old legitimately kicks my ass in her memory card matching game on a daily basis.
I spent the next couple of days there doing the actual neurofeedback treatment and left NYC with a computer to take back home to Arizona. I spent the next month and a half doing virtual neurofeedback treatments. From Monday-Saturday, I would spend Ryan's afternoon naps with headphones on and electrodes on various locations on my scalp. My response was....bizarre. In the first full week, I had several days in a row of lower-than-normal pain. That was a REALLY big deal. We were all super encouraged. Then, things took a turn. For the next 6 weeks, every day was worse than the last. My pain intensity was reaching new highs and staying at those levels for new lengths of time. Truly terrifying. Dr. Fallahpour was working to tweak the protocols of my treatments and not quite understanding why my brain was responding this way. He explained that in some complex cases, it's not uncommon for the brain to go through an initial "resistance" but that things typically stabilized much sooner. I knew it was important that I gave this a fair shot, but ultimately, we all decided I needed to stop.
A separate potential treatment that we'd initially discussed with Dr. Fallapour was TMS, or trans cranial magnetic stimulation. TMS therapy involves using a magnetic filed to stimulate underactive neurons in specific parts of the brain. It's most commonly used (and FDA approved) for mental health conditions like depression, anxiety, and even certain addictions. There's also research supporting its use in the treatment of chronic pain (though not FDA approved). Back in 2014, my Mayo neurologist, Dr. Dodick, had me try a handheld single pulsed TMS device that he was using in a study on migraines and cluster headaches (a study I didn't qualify to participate in but he was kind enough to let me take home a unit to try). Unfortunately, the single pulsed TMS didn't help me but it's also much different than regular TMS, where you're getting something like 50 pulses per second.
TMS Therapy is a commitment - patients typically undergo treatment for a minimum of 5 days per week for 4-6 weeks. Similar to neurofeedback but I would obviously need to be in office vs remote. So if I do try it, I'll need to wait until Ryan starts school later this fall. I do think it's worth a shot, but I'd be lying if I said my response to neurofeedback wasn't a real blow to my already compromised mental state.
While in NYC, Craig and I made two more stops. (And walked I think 50 miles?) The first was another neurologist who Dr. Fallapour had recommended we see. Dr. Mauskop is the director and founder of NY Headache Center. We were grateful that he was able to squeeze us in on such short notice, but I wouldn't say we came away from the appointment with any novel insights. He agreed my pain is a result of central sensitization and supported my treatment path at the Brain Resource Center. Conversations like these are so frustrating for me. On the bright side, there's an element of validation when doctor's "agree" on something. But it can also feel like what they're agreeing on is "we don't know." It can just feel like gut punch reality check that nobody - not even the best of the best - knows how to really and definitively help me.
Our second stop was a visit with Dr. Dodick, who left Mayo last year to become the medical director at this really incredible concierge medicine clinic that is basically bringing together the world's leading medical minds + cutting edge science and technology with a vision of ultimately democratizing access to preventative medicine on a global scale. (He is just a hell of a doctor). He gave us a tour of their facility and we had a chance to catch up on all that's been going on since I last saw him.
He gave me the name of a neurologist at Mayo he'd want me to see since I do need to reestablish with a new one there. (I've since made an appointment with Dr. Green for December). We also chatted about some pharmacological options that I'm waiting until I'm done breastfeeding to pursue, including monoclonal antibodies. These are human-made antibodies (proteins) that bind to other proteins in your body. In migraine patients, these medications attached to calcitonon gene-related peptide (CGRP), which is a protein that can impact migraines by widening blood vessels in the brain. He also told us about new research into microdosing with psilocybin (i.e. magic mushrooms) and lysergic acid diethyalmide (i.e. LSD) to treat migraine and cluster headaches. Again, I'm not a typical "migraine" patient, but without the luxury of a meaningful diagnosis, I just can't afford to leave any stone unturned.
Let's see. What else...
In late summer, I found myself reading more and more about CSF leaks. Not a new topic for me - remember I said we had ruled out a leak back in 2013? I had mentioned Dr. Scali in my last post - the researcher who had first reported the myodural bridge (the tissue connecting the suboccipital muscles and cervical spinal dural mater) back in 2011. He had just recently published and kindly shared with me his manuscript titled The relationship between the myodural bridge, vertebrodural structures, and idiopathic cerebrospinal fluid leaks in whiplash injuries. I became convinced that there just has to be something going on with my CSF that explains not only my response to cranial sacral therapy but my lack of response to...virtually everything else? I scoured the internet reading story after story of CSF leak patients who didn't fit the classic symptoms of a leak: orthostatic headache (meaning the pain is severe when upright but disappears when lying flat), clear fluid leaking from nose or ear, etc.
I contacted a neurosurgeon at Cedars-Sinai, Dr. Wouter Schievink, director of the Cerebrospinal Fluid Leak program, who I had learned was the go-to guy. I compiled a decade's worth of medical records - no small feat - and mailed them to Cedars. He would review them (free of charge, which is so kind) and let me know if an in-person visit was necessary. Six weeks later, I was leaving a Mommy and me playtime at a local gymnastics gym. I buckled Ryan in then did that thing that all parents do where you check at least two things off your day's to-do list in the walk from the backseat around the trunk to the front (IYKYK). I had an email from Dr. Schievink in my inbox. I held my breath as I read the words. "I see no evidence of a CSK leak." FUCK. I felt that familiar lump in my throat as I fought to hold back tears.
Don't get me wrong. It should be a relief to know I don't need a epidural blood patch or another neurosurgery but at this point I am just so, so, SO desperate for an answer.
A few months back, I had scheduled an appointment with a local neurologist, Dr. Rau, who's a member of the Spinal CSF Leak Foundation's advisory board. Her name had come up in some of the online CSF leak groups so I got on her calendar at the soonest availability, which is October. In his email, Dr. Schievink noted that she's an outstanding headache doctor and very knowledgeable about CSF leaks, so it of course never hurts to get another opinion. He also mentioned that most spontaneous CSF leaks are located in the thoracic spine (most of my imaging has been cervical).
So.
That's kind of where I'm at right now. Many days (and nights, unfortunately) are brutal. Others are more manageable than others. As always, there's no real rhyme or reason to it, which is just a real mind fuck. (Sorry, I just googled a synonym for "mind fuck" but it turns out this is the best way to communicate the feeling). I try to stay focused on what I can control. My routine and environment are a big part of that. But unfortunately, they're not enough. The majority of mornings, I wake up with a vice grip around my head. Drills going through my temples. A deep and unrelenting ache into my eye sockets, across my forehead, and over the top of my head. The feeling like someone has taken a baseball bat to the base of my skull. And that, friends, is how my day starts. I work out first thing because feeling stiff seems to just take things from worse to whatever is worse than worse. And then I cold plunge. From there, it's full steam ahead because it's the only option there is. The second Ryan is down for her nap in the afternoon, I'm back in bed with my ice packs. When I sleep at night, it's not uncommon for me to cycle through 6-8 of them before morning.

Chronic pain weaves this complex web through every facet of your existence. And with every passing hour, day, week, month, and year - you feel more tangled in it. Trying to find the balance of living and enjoying life while constantly and carefully monitoring where and how I spend my energy in order to not suffocate from physical pain is ... exhausting, consuming, depleting. And also just my reality.
Just last weekend, Craig, Ryan and I grabbed an early lunch at a local fast casual restaurant. We arrived just after they opened at 11 am and were quite literally the only people inside. But the music from their speakers was loud. I had already woken up with high pain, but by early afternoon, the spike was just out of control. Should I go to the ER right now? Their migraine infusions have never helped me. So I don't go.
Despite all that bullshit, I whole heartedly believe that the worst thing that someone in chronic pain can do is exist solely as a person in chronic pain. So I lean in with all my might to every other part of my life. Mostly, my role as Mommy. I soak up every waking moment with Ryan. We play, we read, we cook, we ride bikes, we chat, we swim, we color, we do science experiments, we run errands, we go on adventures, we do nothing, we do everything. And I am just so grateful to have this fleeting time with her. Parenting may be hard work, but for me, motherhood is not the struggle. It is the escape. And if my eyes don't well up every time she puts her hand on my arm and asks me how my head is doing.. Just this morning Craig stood behind my chair at breakfast to rub my neck for a few minutes. No words had been spoken to her about the morning I was having but Ryan looked at me and in her sweet, gentle voice said "Mom, I'm sorry you're not feeling good."



 |
Craig and I have also spent the last year writing a children's book, which we're currently in the process of publishing. We are so excited about this book. It's been quite a learning experience and a real labor of love. Stay tuned for more on that!
I'll wrap up this already-too-long-of-a-post with a final thought. I recognize that it's hard to support someone battling pain the way I am. Of course it's never easy to watch someone you care about suffer, but the support system protocol is a little more intuitive following an acute injury or recovering from a surgery, let's say. But a random Tuesday afternoon in the 132nd month of their headache? There's no handbook for that. (Although if there was, it'd be because my husband wrote it.) I'm so lucky to be loved and cared for so hard by Craig. He supports me in every possible sense of the word - in ways you can't possibly know exist unless you've endured something like this. But I also realize that when you don't know what to say to someone who is suffering, the path of least resistance is to say nothing at all. I get that. So I'm incredibly grateful for the people in my life - some I know well, and some hardly at all - who make the effort to overcome the discomfort or uncertainty of saying the "right" thing and just say something. Please know how much I appreciate you.