It's been a busy and hard few months working on this head of mine. Pain hasn't let up. Excruciating hours turn into days turn into weeks turn into new baseline levels of pain. And all the while, life goes on. All the good parts shine through (sometimes even brighter). But the sheer agony of chronic pain; all the fear, anxiety, and hopelessness it carries...it takes no days off. It's all-consuming yet for me entirely invisible to you. It is suffocating and overwhelming and terrifying in a way I can't fully explain. So I keep searching for answers because, well, there really is no other option.
So here we go.
Treatment update
In my last post, I recapped the treatments I'd been undergoing in the last six months or so. I stopped Shockwave soon after that, as we weren't able to recreate or even come close to the soft tissue changes it seemed elicit back in January. Similarly, after about six weeks of daily use, it was apparent that the Light Stim red light therapy bed also was not having any impact on my pain levels. If anything, it seemed to exacerbate my symptoms, which makes very little sense but also isn't entirely surprising based on the response I've had to other laser treatments in the past.
Per the last recommendation from my neurologist, Dr. Dodick, I mentioned trying a course of N-acetylcysteine (NAC), which is a precursor molecule to the body's main antioxidant, glutathione, and has been studied in traumatic brain injury patients for its neuroprotective and mitochondrial-boosting benefits. Along the same lines, I underwent three NAD+ infusions with my naturopath this spring. NAD+ (or nictotinamide adenine dinucleotide) is what fuels metabolic reactions and is used therapeutically to to treat a variety of age-related, inflammatory, autoimmune, and neurologic conditions. Unfortunately, I didn't experience benefit from any of it.
A fractured C2?
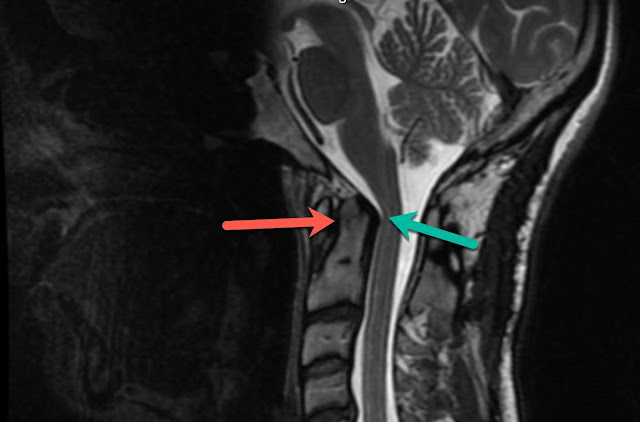
I also mentioned that my current pain doctor, Dr. O'Connor, had referred me to a new neurosurgeon, Dr. Hamid, just to get a fresh perspective as we continue plowing through what's left of interventional pain management procedures. Was there some other big piece of the puzzle we were still missing? I had a new head and neck MRI prior to this appointment just to ensure we had the most up-to-date information. Dr. Hamid agreed with Dr. Dodick's Complex Regional Pain Syndrome diagnosis, especially after seeing photos of some of the red spots on the back of my neck (see last post). And here's a more recent one below.
But he also pointed out something really interesting: an old fracture at C2. Of course we can't prove it to be true, but given that my whiplash bike accident was the event that started this all, causing severe ligament damage and instability at C1/C2, we have to assume that I did indeed break my vertebrae when I hit that tree. You can see the lighter line that runs horizontally across the top of my second cervical vertebrae, in between the arrows. It blows my aching mind beyond belief... of all the expert eyes that have seen this imaging over the last 10 years, not a single doctor or radiology report has identified the fracture. How is that even possible?
The good news is that the fracture has healed well so he doesn't think it's causing any issue, but interesting to note nonetheless. And other than that, he didn't really have other insights or recommendations, aside from an implanted neurostimulator. I think I've written about these before, probably before my occipital nerve surgeries. Essentially, this consists of a neurostimulator device implanted under the skin with wire leads that deliver electrical pulses to the epidural space near the spine. You control the impulses with a handheld device, with the goal of controlling pain by disrupting the pain signals that travel between the spinal cord and brain.
I've learned to never say never, and if you've been around here long enough, it's fairly obvious that I'll cut open any part of my body wide open if there's a chance it could help my head. But, from the research I've done and the experiences I've had with nerve stimulation, I'm just not convinced right now that this is the right path to pursue.
More therapies and procedures
Back in April, Craig and I consulted with a physical therapist, Dr. Turner, of Texas Migraine Clinic. We really liked Dr. Turner. His approach to cervicogenic migraines targets the cervical spine at lower levels than most doctors. In his experience, he's found C5/6, C6/7 as primary pain generators. So he led me through a series of simple (and supported) cervical extension movements with the goal of basically "milking" the disc forward to alleviate irritation of nerves traveling up the brainstem. I tried the exercises for a period of time but unfortunately, didn't experience any shift in pain. If anything, my pain spiked. As it does.
Now on to the interventional procedures I've had with Dr. O'Connor since March.
The day after my last post, I had an occipital nerve block. This was one of those desperate "let's triple check this just in case" procedures. As I explained before, the only real substantial relief I've ever had from a procedure, whether diagnostic or therapeutic, were my ON blocks with Dr. Peled in San Francisco prior to my first decompression/excision surgery in 2017 (even though the surgery itself did not help). This time around, the blocks provided no relief. But I guess worth trying, right?
On that note, we are planning to fly back to San Francisco this summer to try another round of blocks with Dr. Peled. Craig and I spoke to him a few weeks ago just to pick his brain about all that's going on. We both just can't shake the fact that I responded so well to those injections.
He recommended a few things:
First, that I try a scalene block. If there is nerve pain being generated by my brachial plexus, this has some potential to help. If brachial plexus sounds familiar, it's because that's actually one of the spots Dr. Centeno is planning to reinject my stem cells into when we FINALLY are able to get back to Grand Cayman. (Side note update on that: they're hoping for September reopening). I've never had a scalene block before though, so I am (of course) on board to try.
Next, that we try finding another peripheral nerve target to treat. Dr. Peled explained that in about 10% of patients he operates on, he finds an aberrant lesser occipital nerve branch located next to the trapezius muscle (vs. behind sternocleidomastoid). As a reminder, he decompressed my lesser ON in the first surgery, but there's a chance I could fall into that minority group. I think it's at least worth having him block my lesser ON just to see how I respond.
Okay, back to Dr. O'Connor. Man, I am really all over the place right now. But my head feels like it's going to absolutely explode right now so I think this is the best we're gonna do.
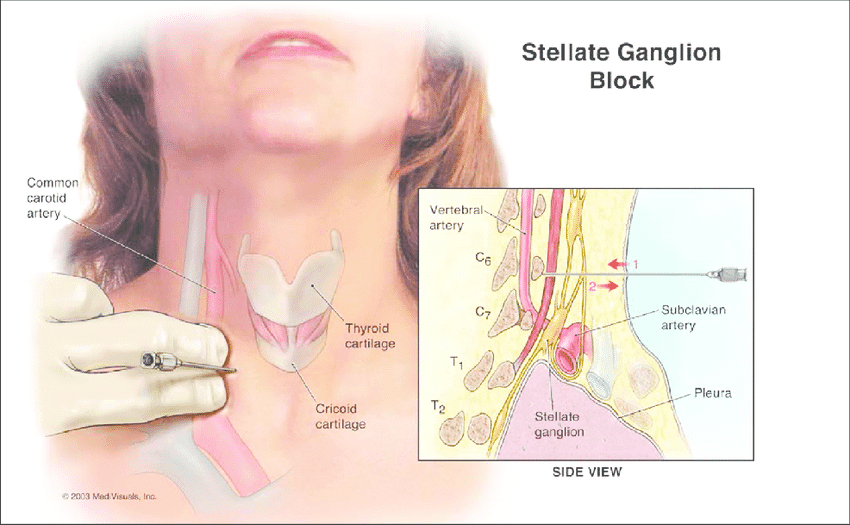
Next on tap with Dr. O'Connor was my first stellate ganglion block. The stellate ganglion is a collection of sympathetic nerves found anterior to the neck of the first rib. It provides most of the sympathetic innervation to head, neck, upper extremities, and a portion of the upper thorax. Blocks are often used to diagnose or treat a variety of circulation problems or nerve injuries, including complex regional pain syndrome (CRPS) and different types of neuropathic pain disorders. They're even used to treat PTSD, which is pretty fascinating.
This was my first nerve block performed face up on the table. The doctor inserts a needle into your neck (on one side of your voice box) and injects a local anesthetic. Then under x-ray guidance, they use a second needle to precisely inject an anesthetic medication. For the rest of the day, it's common to experience things like a temporary droopy eye (which happened after my first) or arm numbness (which happened after my second). The most significant relief should come in a relatively short window following the procedure.
This Friday, I'll go in for my fourth SG block (first right, then left, right again, and now left). I had a little bit of pain reduction from the first two, more so on the left side, but nada from the third. Ideally, we'd love for the relief to build on itself, but that doesn't really seem to be happening so far.
Interestingly, when I lay down on the table for my second SG block and Dr. O'Connor instructed me to turn my head to the right, he was pretty taken aback by the rigidity of my sternocleidomastoid. It's all very normal to me because all the muscles of my neck are always so tight, and coupled with compromised mobility from my fusion, tension is just what I'm used to feeling. But it made him think that it may be worth trying to inject some Botox into those SCMs. Most people know it's used for migraines, but Botox is also a common treatment for cervical dystonia, or spasmodic torticollis. It works by preventing nerves from releasing acetylcholine, which prevents your nerves from sending messages to your muscles telling them to contract or spasm.
I've had Botox injected pretty much everywhere else on my head (aside from the places where wrinkles appear, hah!) so I was immediately on board. Right now, we're just waiting for my insurance to approve it. They like to deny every procedure I have (every. single. one.) which means each one has to go through an appeal process before getting scheduled. If you live in chronic pain, you know the struggle.
NYC for a Brain Scan
To continue chasing down any central contribution to my pain (central sensitization/CRPS), Craig and I will be traveling to New York city next week so I can have a qEEG assessment.A few months ago, we were introduced to a neuropsychologist who has worked with many post-concussion/TBI patients/chronic pain patients. The brain mapping that I'll have done will measure electrical activity in different areas of the brain. From there, neurofeedback can be utilized to up or down-regulate areas of the brain that are over or under-active. We’ll learn a lot more when we’re there about the assessment and interventions that can be used to help normalize anything that's out of balance. So I'll definitely be writing more about that soon.
Thoracic Outlet Syndrome
Lastly, I wanted to share a little of my appointment yesterday with Dr. Broussard, a thoracic surgeon who specializes in Thoracic Outlet Syndrome (TOS). I haven't talked about TOS before, as it's something I've really only explored recently. If you're not familiar, TOS is a condition involving compression of the nerves or blood vessels that pass through the base of the neck. It's typically characterized by disabling pain in the neck and shoulder, along with pain, numbness, tingling, and weakness in the hands and fingers. This obviously doesn't exactly line up with my condition, but over the last few months, I've developed increasing nerve pain down my left arm. The pain is very much connected to what's going on in my neck and up the left side of my head. As my head pain spikes, the nerve pain also increases. So I started researching a little more.
There are three types of TOS: Arterial (compression of the axillary-subclavian artery), Venous TOS (compression of the axillary-subclavian vein) and Neurogenic TOS, or nTOS, (compression of the brachial plexus nerves). I learned that whiplash can also be a cause of nTOS (really any injury that results in chronic cervical muscle spasm). So I started to really wonder if there is a compression in my brachial plexus that's driving pain. (And remember Dr. Peled's suggestion to try a scalene block to target the brachial plexus? And Dr. Centeno's plan to inject my stem cells into my brachial plexus?)
So Craig and I went to see this surgeon here in Phoenix, who happens to be a very well-respected surgeon in the TOS world. And he was wonderful. He spent a solid 90 minutes with us, talking through my history (which is, as you can imagine, a bit of a doozy). He walked us through his diagnostic algorithm, explaining that although nTOS is the most common, it's also the hardest to diagnosis. It starts with a clinical diagnosis to determine whether next steps are warranted: first a dynamic CT angiogram to check for compression and anterior scalene hypertrophy, then Botox injections (under guidance) of anterior scalene and pec minor. From there, surgical options are weighed. Surgical treatment of TOS consists of first rib resection to alleviate compression.
In terms of the headache/TOS connection, Dr. Broussard explained that he does see a connection with occipital headaches, but not as much with pain in the frontal region. On the whole, nTOS symptoms are generally just more distal than central, which was leading him to think it really wasn't an underlying issue for me. I experienced very little reproduction of symptoms during the physical exam (upper extremity tension testing was really the only portion I showed positive signs for), which made him think that additional testing, at least at this time, probably just doesn't make sense.
I felt a mix of emotions leaving his office. Relief, I guess, to eliminate a diagnosis that doesn't necessarily have the easiest pathway to recovery. But also defeat. It's disheartening to be told (even by the most compassionate of doctors, like Dr. Broussard) that he can't help you.
But, I'll continue focusing on what's ahead. Hopefully these next few months will bring some new insights and positive treatment outcomes. As Ryan likes to say when she takes a spill on her Strider bike (before I can even ask if she's okay)...
As someone who has had this problem, I think it is plausible that the headache emerges from the neck area (cervicogenic headache). One clue is that the surrounding tissue is quite tense. Palpate the area to check for knots and very firm, tense muscles along the neck and back of shoulders, scapula etc. Look for shoulders that hang out at a 90 degree angle instead of being sloped, as well as shoulder and arm pain (TOS). The solution to these findings may be to stretch and learn to relax these muscles, as after a head and trauma, the neck tends to protect this area by engaging these muscles, sometimes causing muscle spasms, which in turn irritate the occipital nerves, running up the skull and producing a "headache" occipital neuralgia. If this is your problem, it may take more than six months of rehabilitation exercises, but in my case it helped. I do not have ON, but still some residual neck pain.


Sent you a private message on FB. Thinking of you. Cousin Nancy
ReplyDeleteAs someone who has had this problem, I think it is plausible that the headache emerges from the neck area (cervicogenic headache). One clue is that the surrounding tissue is quite tense. Palpate the area to check for knots and very firm, tense muscles along the neck and back of shoulders, scapula etc. Look for shoulders that hang out at a 90 degree angle instead of being sloped, as well as shoulder and arm pain (TOS). The solution to these findings may be to stretch and learn to relax these muscles, as after a head and trauma, the neck tends to protect this area by engaging these muscles, sometimes causing muscle spasms, which in turn irritate the occipital nerves, running up the skull and producing a "headache" occipital neuralgia. If this is your problem, it may take more than six months of rehabilitation exercises, but in my case it helped. I do not have ON, but still some residual neck pain.
ReplyDeleteJust curious: Do you see any imaging artifacts on your MRI, as a result of the metal hardware (screws) from your surgery?
ReplyDelete